
Photo: Health campaign in Bangladesh. Credit: Maruf for Children Without Worms, Task Force for Global Health.
Linksbridge SPC conducted a study on health campaign integration that examined reasons for, characteristics of, and influences on full and partial integration.
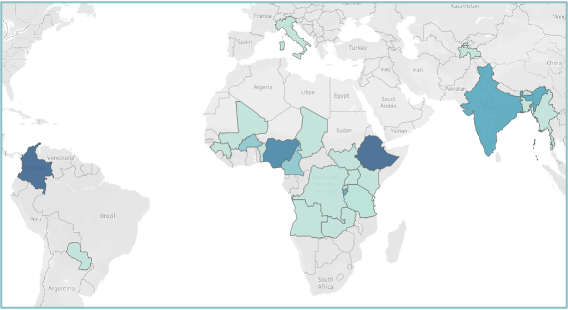
Countries are represented across 4 WHO regions (Africa, Americas, Europe, Southeast Asia)
To contribute to existing data on partially and fully integrated health campaigns around the world, Linksbridge SPC conducted a mixed-methods study that included participants who reported on campaigns in 26 countries, and across several health domains. The research comprised collection and validation of health campaign integration data with a focus on the geographies with integrated campaigns, as well as levels of, reasons for, and influences on such integration.
As countries work to recover from the disruption of health campaigns by the COVID-19 pandemic, stakeholders show a renewed interest in health campaign integration. Such integration can occur fully or partially. In full integration models, partners collaborate, share tools and resources, and co-deliver interventions, whereas partial integration involves the former elements without the co-delivery of services.
The existing data on integrated campaigns focus on full integration, with minimal data available on partially integrated campaigns. In response to this gap in information, Linksbridge SPC aimed to provide a better understanding of integrated campaigns through the data gathered for this study.
The objectives of this study were to:
The data from this study reflect that campaign integration—especially partial integration—occurs more frequently than previously documented. For the 26 countries represented in this study, partial integration was the most common type of integration. Campaign integration occurred across all disease areas at various geographic levels. The ease of integration varied by the types of campaigns. Campaign managers favored campaign integration under appropriate conditions, with consensus among participants that national health policies and strategies should include integration considerations.
Heather Ferguson of Linksbridge SPC walks through the background, methods, results, and lessons learned from the campaign integration study.
See the slides for more characteristics of integrated campaigns